Impairments
What is an “impairment” and why might you model one?
Understanding the definition of an impairment can be difficult, especially since it’s an artifact of data availability in the GBD modeling process. A more in depth definition for impairments and how this relates to other GBD terms defining disease can be found on this GBD health page.
In short, sometimes GBD has a lot of information about an overall condition that the modelers want to utilize. However, the information typically couldn’t be included in the cause hierarchy since the impairment has more than one cause. Therefore, modelers include it as an impairment.
An easy example to grasp is blindness. There is a lot of data available about blindness, but it can be caused by a lot of different things. Therefore, it is difficult to place in the cause hierarchy, but we want to include all the rich data we have. Hence, it is an impairment.
Modeling impairments can be important for a simulation depending on the research questions. Continuing the blindness example above, if you wanted to include an intervention that targets blindness generally, you would ideally want to include blindness, but wouldn’t necessarily want to include all of the possible causes for blindness. Hence the need to model the impairment instead of all causes of the impairment. Including all of the causes would unnecessarily complicate the model and include information not relevant to our research question.
On the other hand, if we were investigating an intervention that targets diabetes, we might not need to include blindness as an impairment. Instead we could just track the sequela “blindness due to diabetic mellitus” since we are only concerned about blindness due to a single cause.
It is important to think through your research question and what is being affected by your interventions to determine if including an impairment is needed.
Comparing and Contrasting Impairment and Cause Models
In general, modeling impairments is similar to modeling causes - they are both medical conditions simulants can experience. Therefore, most of the cause modeling page is still applicable and should generally be used for modeling impairments.
However, there are a few important differences between modeling causes and impairments that we will cover here. These differences largely pertain to data sources and availability.
Disease Models
The GBD data availability differs by impairment significantly. For example, heart failure has an incidence, prevalence, excess mortality rate, and disability weights. Therefore, you could create a heart failure model more of less exactly as you might make a cause model.
On the other hand, anemia does NOT have an incidence or any mortality associated with it. It does have a prevalence and disability weight. Therefore, other methods might be needed in order to have a dynamic anemia model. You can see one example of this based on simulant’s hemoglobin levels in the hemoglobin, anemia and iron deficiency model.
Another option would be to derive the needed values from cause level data. You could aggregate incidence or another needed variable from all their causes, weighted by prevalence of their sequelae in the impairment. This might require working with the relevant GBD team to get any data available on sequelae included in the impairment and proportion of each cause.
Risk Models
GBD does NOT include relative risks or PAFs connecting risk factors to impairments. Therefore, if you need to model the impact of a risk factor to an impairment you will need to use literature values for relative risks. These values might have limitations. For example, check the study population used to find relative risks to ensure it is applicable to the full range of risk factor values - sometimes you might need to cap the relative risks if the study does not apply to very high risk factor values.
After you have defined the relative risks you plan to use, you will need to recalculate the PAFs to include this new “cause” in the model. More information on PAFs can be found on the measures of risk page.
Once you have a completed model design, take care to include model updates one step at a time with V&V between each step. Mixing data sources and generating model data can introduce opportunities for error, so checks along the process are important for success.
Techniques for Modeling Impairments and Causes Together
The above section goes through the basics of adding an impairment to your model. But what happens if you want to include both a cause and impairment that overlap?
Let’s return to our blindness example from above. What if you want to include both blindness as an impairment AND diabetes as a cause? We can imagine a few possible solutions, each of which has pros and cons. The “right” answer for how to model impairments in your simulation will depend on the requirements and data available.
Include Both Cause and Impairment Separately
One solution would be to include the cause and impairment as separate model components. However in this case blindness and diabetes overlap - they both include the sequela “blindness due to diabetes mellitus” in their GBD prevalence and incidence rates. So including both separately would double count this sequala.
If they overlap is small - say diabetes only causes 1% of all blindness - this might be an acceptable limitation of the model. However, usually this would not be favorable modeling plan.
Since you can define the size of the overlap, it is a sequela with data after all, you might try and “subtract out” the overlap from one model or the other. For example, you could include diabetes as listed in GBD, and define blindness as “blindness due to other causes”, removing the part that overlaps with diabetes.
This would help, but you still have an issue because causes in Vivarium (and impairments!) are assumed to be independent. Therefore, it is possible for a simulant to have both “blindness due to diabetes” and “blindness due to other causes” simultaneously, which should be impossible in the GBD structure.
This would lead to undercounting the total amount of blindness in the population since causes that should be mututally exclusive are not. Again, depending on the size of the overlap this might be an acceptable limitation. It may also depend on risk effects included for both models - if the same simulants are at high risk for diabetes and blindness, the issue would be more exacerbated than if different risk factors caused each.
One example of this can be seen in our IV Iron Simulation and more specifically in modeling anemia and maternal hemorrhage. In this case, YLDs for maternal hemorrhage were not counted due to overlap with anemia YLDs. The anemia YLDs included both those due to both maternal hemorrhage and other causes.
Include All Possible Causes
Another solution might be to include all of the causes that touch blindness, which would therefore include all of the blindness sequelae that make up the impairment. In this approach you would not model “blindness” as an impairment, but could get all of the same data from sequelae.
For the case of blindness, there are approximately 15 separate causes, not including all neonatal causes. This would mean having 15 cause models included! This is likely to be a lot of work, and would probably not provide much extra information.
Furthermore, you still have the issue that cause models are independent in Vivarium. Simulants could still get blindness due to multiple causes, leading to the same undercounting of total blindness.
For practical and logistic reasons, this approach is not recommeneded.
Include a Hybrid Cause & Impairment Model
Another option is to include a single cause model that includes both the cause and impairment. One example of this is in the CVD model where IHD and Heart Failure are included in the same cause model.
By including both the cause and impairment in a single modeling component, they are no longer independent which solves our prior problems of overlap. In addition, you can define part of the model to overlap - for example states could include diabetes, blindness due to diabetes, and blindness due to other causes.
Including cause models structured in this way does sometimes lead to strange “predictive” qualities for simulants. For example, a simulant with blindness from other causes might not be able to develop diabetes to avoid overlap with blindess due to diabetes. In real life, these conditions exist separately, but can’t in the model.
This approach should not create bias in your model and generally works well. However, if you want to include many causes that overlap with an impairment (e.g., including diabetes, meningitis, glaucoma, and vitamin A deficiency, all of which cause blindness) using this approach would make an extremely complex single “cause” model that likely wouldn’t be feasible to create or V&V.
Therefore, considering your modeling situation and the requirements is important in choosing your modeling approach.
Have Causes Act as “Risks”
Note
While we think this methodology will work well, it has not been tested in a model up to this point. Therefore the implemenation remains theoretical, and some details to the approach would need to be finalized before it could be used.
Another option is to have cause models that act as “risks” on the impairment model. In effect, we would adjust the incidence of the impairment to remove the impact of all modeled causes. This is very similar to how we currently include mortality in our models.
For mortality, a simulant can die due to all cause mortality at any point, or they can die due to a specific cause in our model. Therefore, we decrease the background all cause mortality rate in the model to account for the presence of causes with increased mortality rates. For more information on the math behind this, see the mortality hazards section of the cause model page.
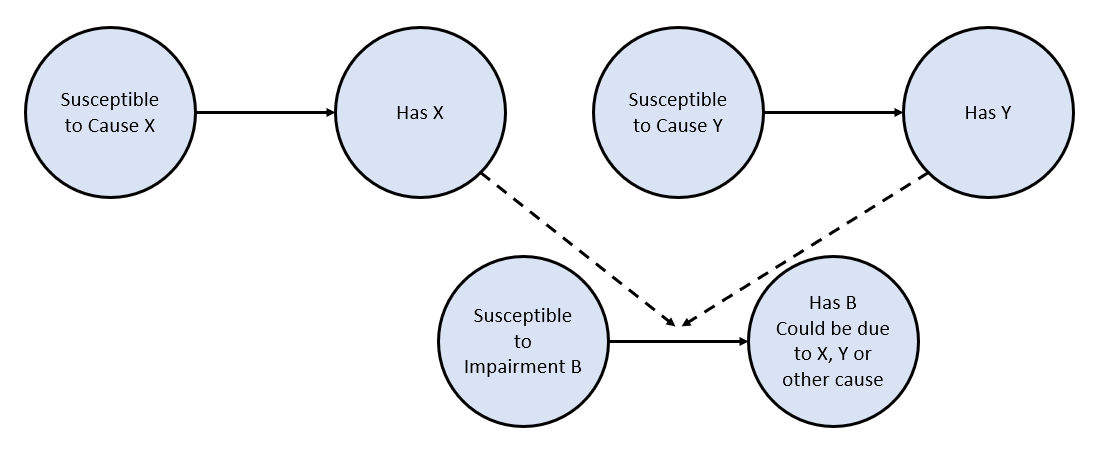
A similar principle can be used here. Referring to the figure below, we can see that two causes, X and Y, act on the incidence of an impairment, B. Since simulants can get impairment B through the causes X and Y, we need to decrease the overall incidence of B to account for the other model factors.
The amount that the incidence of B is impacted will depend on the causes present in the model and the amount of B caused by modeled causes vs other factors. The math for this will largely follow the math for mortality, but has not been designed or tested in a model. If the adjustments are done correctly, this approach shouldn’t create bias in the model and is a good option if you need to include more cause models in the simulation.
If the impairment needs to include remission (e.g., an SIS model instead of an SI model), the analogy to mortality breaks down, and this approach might not be appropriate.