MNCNH Portfolio
Abbreviation |
Definition |
|---|---|
ACMR |
All-Cause Mortality Rate |
ACS |
Antenatal Corticosteroids |
AI ultrasound |
Artificial Intelligence assisted ultrasound |
ANC |
Antenatal Care |
ASFR |
Age-Specific Fertility Rate |
BEmONC |
Basic Emergency Obstetric and Newborn Care |
CEmONC |
Comprehensive Emergency Obstetric and Newborn Care |
CPAP |
Continuous Positive Airway Pressure |
CSMR |
Cause-Specific Mortality Rate |
ENN |
Early Neonatal |
GBD |
Global Burden of Disease |
IFA |
Iron and Folic Acid |
IFD |
In-Facility Delivery |
IV iron |
Intravenous iron |
LBW |
Low Birth Weight |
LBWSG |
Low Birth Weight and Short Gestation |
LNN |
Late Neonatal |
MMS |
Multiple Micronutrient Supplements |
MNCNH |
Maternal, Newborn, and Child Nutrition and Health |
OL |
Obstructed Labor |
PAF |
Population Attributable Fraction |
PPD |
Postpartum Depression |
PTB |
Preterm Birth |
RDS |
Respiratory Distress Syndrome |
RR |
Relative Risk |
RT |
Research Team |
SBR |
Stillbirth (to live birth) Ratio |
V&V |
Verification and Validation |
WRA |
Women of Reproductive Age |
YLDs |
Years Lived with Disability |
YLLs |
Years of Life Lost |
1.0 Overview
This document is the overall page for the Maternal, Newborn, and Child Nutrition and Health (MNCNH) Portfolio simulation and contains information that relates to all modeled subcomponents included in the simulation.
2.0 Modeling aims and objectives
The MNCNH Portfolio simulation builds on work our team has done in other simulations of pregnancy and early childhood. The most recent was the Nutrition Optimization (NO) simulation, which (as the name suggests) focused particularly on nutrition interventions. That simulation allowed us to estimate the impacts of each intervention, and crucially also how the interventions might interact, for example due to prevention reducing the need for treatment down the line. “Optimization” refers to the fact that we used the output of the NO sim to calculate optimal allocation of money to have the biggest impact given a budget, taking all these interactions into account.
Nutrition interventions continue to be included in the MNCNH portfolio sim, but the “portfolio” is broader; the intervention space includes more products. These products, like the nutrition interventions in the NO project, interact in complex ways, and an aim of this simulation is to estimate the impact of different combinations of these interventions. As before, we also plan to estimate costs and calculate optimal budget allocation, possibly with improved costing methodology. This page serves as documentation for the simulation part of the project, which is focused on estimating burden under a variety of scenarios designed to surface all the relevant product interactions.
Simulating more interventions means simulating more risks and causes for those interventions to act on, simulating more details of the healthcare system to model how those interventions would be delivered, and including more detail in the intrapartum (labor and delivery) and neonatal time periods.
We plan to complete this work in 3 waves.
Wave 1 will include the basic model design, outlines of the healthcare system, and some interventions (AI ultrasound, RDS management).
Wave 2 will add in some antenatal supplements (MMS, IV iron), the hemoglobin risk for birthing parents, all downstream causes affected by hemoglobin, and higher level delivery facility interventions.
Wave 3 will add in gestational blood pressure and relevant causes and risks including pre-eclampsia care and downstream effects of high blood pressure.
As of August 2025, Wave 1 is mostly complete in both documentation and implementation, and Wave 2 is partially documented and has just started implementation.
3.0 Concept model diagram and submodels
As in the NO simulation, rather than simulate an entire population of all ages and sexes, this simulation includes only pregnant people and the neonates they give birth to. We start the simulation with a cohort of simulants all at the beginning of pregnancy, and move them in lockstep through their pregnancies. For those pregnancies that result in a live birth, we then simulate a neonate (we do not model twins) through the first month of life. In this way, our simulation represents all the people who may benefit from the interventions of interest, without wasting computational resources on simulating irrelevant people, such as adult males. We call the potential simulant pair we follow through the simulation (pregnant person and neonate) a “simulant dyad.”
This model is different than NO and other simulations we’ve done in that it follows a decision-tree-like format in which we jump directly to from one decision point to the next rather than taking equal-sized steps through time. For this reason, throughout this model we calculate and express events in terms of probabilities, rather than rates per person-time or similar.
The overall simulation model is divided into four “components,” which are differentiated by the timespan and the simulant that they model.
The Pregnancy component, which models from the beginning of pregnancy until the start of labor.
The Intrapartum component, which models labor and delivery, including delivery complications.
The Neonatal component, which models the first month of life for newborns.
The Postpartum component, which models the six weeks after the end of pregnancy for the pregnant person.
Warning
When we say “component” here, we mean something distinct from a Vivarium component.
Graphically, the component breakdown looks like this:
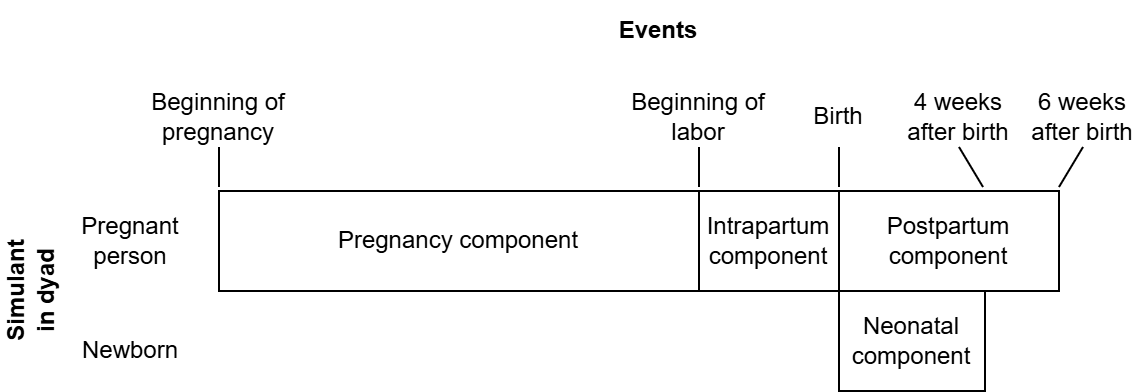
Note
Do not interpret the x-axis in this diagram as time, since e.g. the duration of pregnancy is not at all constant. Also, if misinterpreted this way, the x-axis would be wildly not to scale.
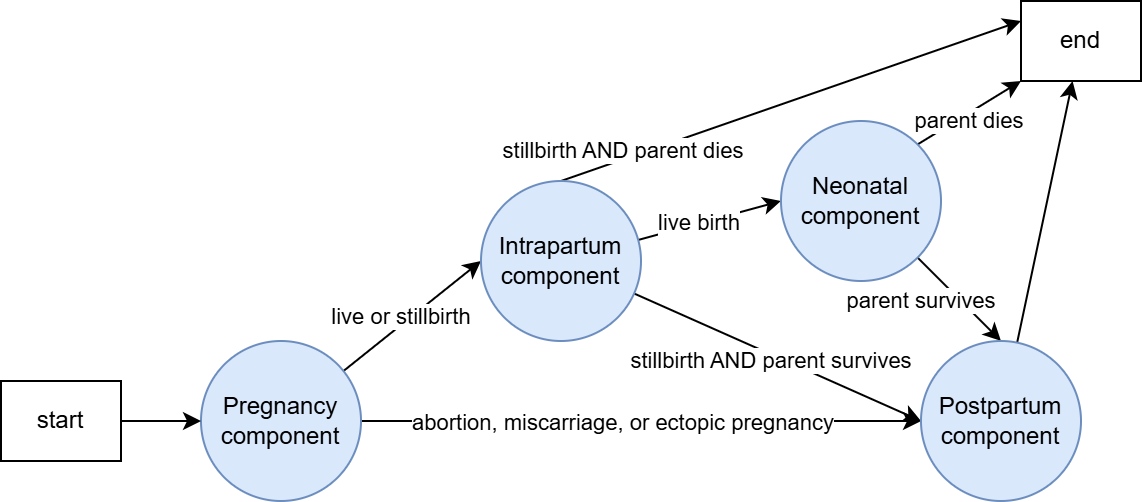
However, the only situation in which all components are actually reached for a given simulant dyad is the case in which the pregnancy results in a live birth and the birthing person survives childbirth. In other situations, some components will not be reached. The rules by which components flow into other components are as follows:
All simulant dyads start at the pregnancy component.
If the birth outcome from the pregnancy component is a live or stillbirth (NOT abortion/miscarriage/ectopic pregnancy), proceed to the intrapartum component. Otherwise, skip to the postpartum component.
At the end of the intrapartum component, if the birth outcome from the pregnancy component is a live birth, proceed to the neonatal component. Otherwise, if the birth parent survives childbirth, proceed to the postpartum component.
At the end of the neonatal component, if the birth parent survived childbirth in the intrapartum component, proceed to the postpartum component.
Here is a graphic representation of the same information:
Each component is further subdivided into “modules,” which are organized by topic (rather than by time/simulant as in the components). Each module may have some simulant dyad attributes as input (values it needs) and some simulant dyad attributes as output (values it initializes). Module outputs may be used as inputs to other modules and/or serve as information for verification and validation and/or simulation results. For clarity, in the tables below we will write the modules in an order that satisfies the following property: each variable is defined as a module output prior to being used as a module input. This helps us make sure we aren’t creating any cyclic dependencies. Technically, any order satisfying this property is an equivalent, valid order in which the modules could be run in the simulation.
Note
There is a template to use when creating new module pages.
Pregnancy component
Module |
Inputs |
Outputs |
Nested subcomponents |
|---|---|---|---|
|
|||
|
|
||
|
|
||
|
|
||
|
|
||
|
|
||
|
|
||
|
|
Intrapartum component
Note
Only live births or stillbirths (NOT abortions/miscarriages/ectopic pregnancies) will proceed to the intrapartum component, as described above.
Warning
As currently designed, the intrapartum component models an intervention for misoprostol to prevent postpartum hemorrhage (PPH) in home birth settings only. We do not consider any interventions for PPH prevention at facility settings nor do we model the expected greater incidence of PPH in home settings relative to facility settings.
Therefore, as written, the incidence of PPH by delivery setting will be miscalibrated to the expectation in reality. We plan to continue with the implementing the model as written while noting this limitation until we implement a strategy to address this (see related ticket here)
Module |
Inputs |
Outputs |
Nested subcomponents |
|---|---|---|---|
|
|
||
|
|
||
|
|
Neonatal component
Note
Only live births proceed to the neonatal component, as described above.
Module |
Inputs |
Outputs |
Nested subcomponents |
|---|---|---|---|
|
|
Postpartum component
Module |
Inputs |
Outputs |
Nested subcomponents |
|---|---|---|---|
|
|
||
|
|
||
|
|
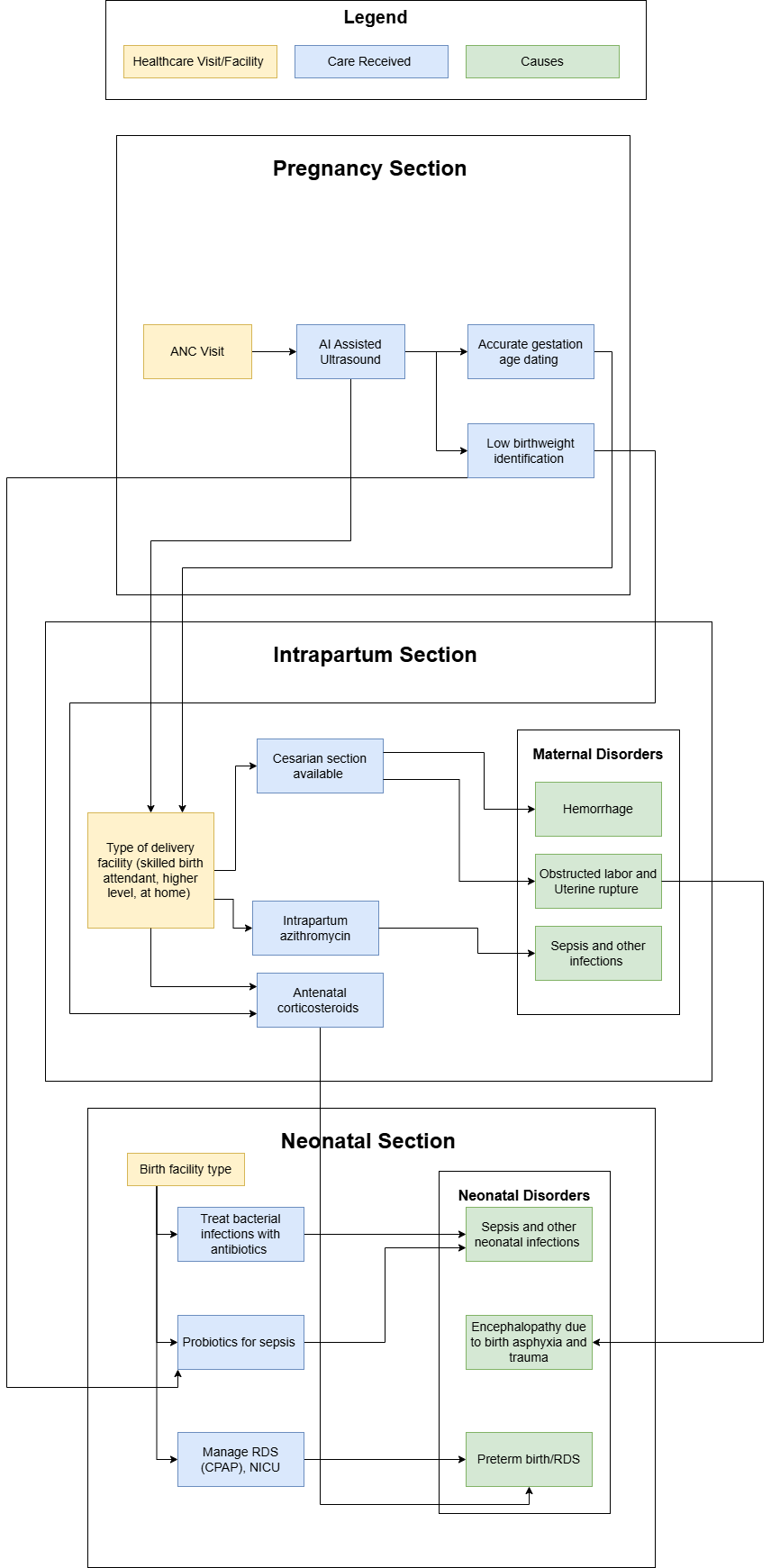
Wave 1 Concept Model Map (has not been updated recently):
3.1 Scenario information
Note
Scenarios were reworked for model version 18.4. To see the definition of scenarios used for prior models, see the record in this pull request. Note that scenario design for this simulation is expected to undergo an additional future rework to achieve compatibility with an “emulator” design.
Scenario |
Ultrasound coverage |
Ultrasound type |
Oral iron coverage |
Hemoglobin screening coverage |
Ferritin screening coverage |
IV iron coverage |
Note |
|---|---|---|---|---|---|---|---|
|
Defined in the baseline coverage section of the AI ultrasound module page |
Defined in the baseline coverage section of the AI ultrasound module page |
Defined in the baseline coverage section of the oral iron supplementation page (use the |
Defined in the baseline coverage section of the anemia screening intervention page |
Defined in the baseline coverage section of the anemia screening intervention page |
Defined in the baseline coverage section of the IV iron page |
|
|
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
100% |
100% AI-assisted |
Baseline |
Baseline |
Baseline |
Baseline |
When compared to 2, shows how AI ultrasound–>facility choice pathway can improve outcomes by having more preterm deliveries deliver in facility settings |
|
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
100% at ANC (no ultrasound among those who do not attend ANC) |
100% AI-assisted |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
100% at ANC (no ultrasound among those who do not attend ANC) |
100% standard |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
100% at ANC (no ultrasound among those who do not attend ANC) |
100% AI-assisted |
Baseline |
Baseline |
Baseline |
Baseline |
Not including anemia related interventions in this run as implementation of all model components is incomplete as of October 2025 |
|
Baseline |
Baseline |
100% MMS |
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
100% |
100% |
100% |
|
|
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
100% at ANC (no ultrasound among those who do not attend ANC) |
50% standard US, 50% AI-assisted US |
Baseline |
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
100% of eligible population |
100% of eligible population |
Baseline |
Scenario |
Azithromycin coverage |
Corticosteroid coverage |
Misoprostol coverage |
Note |
|---|---|---|---|---|
|
Defined on intrapartum intervention model document |
Defined on intrapartum intervention model document |
Defined on intrapartum intervention model document |
|
|
Baseline |
100% at BEmONC and CEmONC, baseline at home |
Baseline |
|
|
Baseline |
100% at BEmONC and CEmONC, baseline at home |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
100% at BEmONC and CEmONC, baseline at home |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
100% at BEmONC and CEmONC, baseline at home |
100% at BEmONC and CEmONC, baseline at home |
Baseline |
Not including misoprostol scale-up in this run because as of October 2025 we have known calibration issues with our hemorrhage model by delivery facility setting |
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
50% at BEmONC and CEmONC, baseline at home |
0% |
0% |
|
|
0% |
0% |
50% among eligible population (attends ANC and delivers at home) |
|
|
Baseline |
0% coverage at all delivery location types |
Baseline |
see neonatal table for CPAP coverage |
|
Baseline |
100% coverage at BEmONC and CEmONC facilities, baseline at home |
Baseline |
see neonatal table for CPAP coverage |
|
Baseline |
100% coverage at BEmONC and CEmONC facilities, baseline at home |
Baseline |
see neonatal table for CPAP coverage |
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
Scenario |
CPAP coverage |
Antibiotics coverage |
Probiotics coverage |
Note |
|---|---|---|---|---|
|
Defined on the CPAP intervention model document |
Defined on the neonatal antibiotic intervention document |
Defined on the probiotics intervention model document |
Baseline coverage values are delivery facility-specific |
|
100% at BEMONC and CEMONC, baseline at home |
Baseline |
Baseline |
|
|
100% at BEMONC and CEMONC, baseline at home |
Baseline |
Baseline |
|
|
Baseline |
100% coverage |
Baseline |
|
|
Baseline |
Baseline |
100% at CEMONC and BEMONC, baseline at home |
|
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
100% at BEMONC and CEMONC, baseline at home |
100% |
100% at BEMONC and CEMONC, baseline at home |
|
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
|
|
100% coverage at BEmONC and CEmONC facilities, baseline at home |
Baseline |
Baseline |
See intrapartum table for ACS coverage |
|
100% coverage at BEmONC and CEmONC facilities, baseline at home |
Baseline |
Baseline |
See intrapartum table for ACS coverage |
|
0% coverage at all delivery location types |
Baseline |
Baseline |
See intrapartum table for ACS coverage |
|
Baseline |
Baseline |
Baseline |
|
|
Baseline |
Baseline |
Baseline |
4.0 Outputs/Observers
Specific observer outputs and their stratifications may vary by model run as needs change. Modifications to default will be noted in the model run requests tables. Note that the observers and outputs listed here are different from the module outputs above. The outputs of the module are intended to be intermediate values that may or may not be included as observed simulated outputs.
Default stratifications to all observers should include scenario and input draw.
Note
Observers cannot support more than 15 stratifications. Design of simulation observers should take this into account.
Observer |
Default stratifications |
Note |
|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
Included. Confirm this represents “eligible birth counts”? |
|
|
Included. Confirm this represents “eligible birth counts”? |
|
|
Included. Confirm this represents “eligible birth counts”? |
7a. Maternal population counts: hemoglobin-related parameters |
|
|
7b. Maternal population counts: other parameters |
|
|
|
|
Observe the following statistics about the \(\text{ACMRisk}_i\) value described on the neonatal mortality page,
which is implemented as the
All of these quantities can aggregate across seeds in the normal way (summation). |
|
|
Observe the following statistics about the \(\text{CSMRisk}^k_i\) value described on the neonatal mortality page,
which is implemented as the
All of these quantities can aggregate across seeds in the normal way (summation). |
|
|
For each living simulant, take the modeled-cause CSMRisks (same pipelines as used in the previous observer), divide them each by the ACMRisk (same pipeline as observer #8), sum them and then subtract 1. If negative, clip this value to zero. This emulates the factor by which the modeled-cause CSMRisk exceeds ACMRisk, requiring a hack to prevent other-causes CSMRisk from being negative. Then observe:
All of these quantities can aggregate across seeds in the normal way (summation). |
|
|
Inclusive of anemia YLDs accrued during pregnancy and the postpartum period |
Todo
Determine whether we want to continue to have duplicate information like:
Stratifying the birth observer by neonatal interventions,
AND separately observing neonatal intervention counts
5.0 Model run requests
Parameter |
Value |
Note |
|---|---|---|
Location(s) |
|
|
Number of draws |
10 |
See next row for which specific draws to be used. Based on calculations from the Nutrition Optimization project: production run number divided in half for default V&V runs |
Draw numbers |
115, 60, 118, 197, 79, 244, 22, 167, 146, 71, 28, 156, 94, 170, 109, 26, 35, 114, 178, 127 |
The standard number of draws available for most of our model input parameters is 500 for GBD 2021 and 250 for GBD 2023. There are a few instances where our input data have different numbers of draws available. Those instances are summarized in the table following this one. To account for the varying number of draws available for our input data, we will pre-specify which draws to select according to the numbers listed here. 20 draws have been listed although the default number of draws for V&V model runs is 10 - the first 10 numbers in this list should be used for V&V runs. This list of numbers was first generated for GBD 2021 data starting in model 11.0 by sampling a random number between 0 and 499 and resampling when a number was generated that had the same remainder after dividing by 100 or 250 as a number that was already in the list. This strategy ensures that we do not run multiple draws that have identical data for any parameter in our model. These draws included: [115, 60, 368, 197, 79, 244, 272, 167, 146, 71, 278, 406, 94, 420, 109, 26, 35, 114, 428, 218]. The final number in the list (218) was updated from (170) in September of 2025 to account for new input data with 250 draws. This list was later updated for GBD 2023 data starting in model 19.0 by taking the remainder of each number in the GBD 2021 list after dividing by 250 and re-sampling a new value for 218 (which had a duplicate value % 100 as another number in the list). |
Population size per draw |
100,000 |
Based on calculations from the Nutrition Optimization project: production run number divided in half for default V&V runs |
Randomness key columns |
[‘entrance_time’,’age’] |
Note that each row of the population table in this simulation contains a pregnant simulant AND the outcome of that simulant’s pregnancy. Therefore, the conversion of a stillbirth to a live birth between simulated scenarios in this simulation will not result in a new row added to the simulation state table and therefore will not change the state table index value of other simulants like occured in the IV iron simulation and resulted in disruptions to common random numbers between scenarios. Therefore, these randomness key columns are expected to be sufficient for this simulation. |
Age start (initialization) |
10 |
Applies to pregnant population only |
Age end (initialization) |
54 |
Applies to pregnant population only |
Age start (observation) |
N/A. All pregnant simulants observed from start of pregnancy. All neonatal simulants observed from birth. |
|
Age end (observation) |
N/A; All pregnant simulants observed through conclusion of relevant modeled outcomes. All neonatal simulants observed until 28 days (end of late neonatal age group) |
Pregnant/birthing simulants do not age in this simulation |
Parameter |
Number of draws |
Strategy for GBD 2021 (Models <19.0) |
Strategy for GBD 2023 (Models 19.0+) |
Note/reference |
|---|---|---|---|---|
Standard GBD data |
500 for GBD 2021, 250 for GBD 2023 |
Use 500 draws as is |
Use 250 draws as-is |
|
Hemoglobin risk exposure (using GBD 2023 data) |
100 |
Copy 5 times so that draw 1, 101, 201, 301, and 401 all have the same value, etc. |
Copy 2.5 times so that draw 1, 101, and 201 all have the same value. Note that draws 0-49 will be used three times and draws 50-99 will be used twice. |
|
Hemoglobin risk effects, including those on stillbirth, gestational age, and birthweight that are modeled through the IV iron intervention model |
250 |
Copy twice so that draw 1 and 251 have the same value, etc. |
Use as is |
Note that we have ordered the draws for hemoglobin RRs on gestational age, birth weight, and neonatal sepsis in the same order as we are modeling mediation by gestational age and birthweight in the effect of hemoglobin on neonatal sepsis and therefore expect that these draws will be correlated. |
100 |
Copy 5 times so that draw 1, 101, 201, 301, and 401 all have the same value, etc. |
Copy 2.5 times so that draw 1, 101, and 201 all have the same value. Note that draws 0-49 will be used three times and draws 50-99 will be used twice. |
Note
The “Directory” column in the table below lists the subdirectory nested within mnt/team/simulation_science/pub/models/vivarium_gates_mncnh/results/ where results specific to that model run can be found.
Model numbers with an asterisk indicate planned model runs that are not yet ready to be implemented.
Number |
Run |
Scenarios |
Directory |
Specification mods |
Stratification mods |
Observer mods |
|---|---|---|---|---|---|---|
1 |
Wave I Pregnancy V&V |
Baseline |
|
|||
2 |
Wave I Maternal disorders V&V |
Baseline |
|
|||
3 |
Wave I Neonatal disorders V&V |
Baseline |
|
|||
3.1 |
Wave I Neonatal disorders V&V with correct LBWSG distribution |
Baseline |
|
|||
3.2 |
Wave I Neonatal disorders V&V with LBWSG component removed |
Baseline |
|
|||
3.3 |
Wave I Neonatal disorders V&V with early NN observer bugfix |
Baseline |
|
|||
4.1 |
Wave I CPAP |
Baseline |
|
|||
4.2 |
Wave I CPAP with observer for counts per facility type |
Baseline |
|
|||
4.3 |
Wave I CPAP with addition of a delivery facility column in births observer and CPAP availability stratification in neonatal burden observer |
Baseline |
|
|||
4.4 |
Wave I CPAP with updated determination of delivery facility type |
Baseline |
|
|||
4.5 |
Wave I CPAP with bugfix for negative other causes mortality rates |
Baseline |
|
|||
4.6 |
Wave I CPAP with scale-up scenarios |
Baseline and alternative scenarios 2, 3, and 4 |
|
|||
4.7 |
Correct pregnancy duration for abortion/miscarriage/ectopic pregnancies |
Baseline and alternative scenarios 2, 3, and 4 |
|
|||
5.0 |
Wave I neonatal antibiotics with scale-up scenarios |
Baseline and alternative scenarios 2 - 7 |
|
|||
5.1 |
Wave I neonatal antibiotics with scale-up scenarios; engineer refactor |
Baseline and alternative scenarios 2 - 7 |
|
|||
6.0 |
Wave I neonatal probiotics with scale-up scenarios |
Baseline and alternative scenarios 2 - 10 |
|
|||
6.0.1 |
Wave I neonatal disorders ACMR with 200k population without interventions |
Baseline |
|
Population increased 10 fold (random seed population size changed from 20k to 200k) |
||
6.0.2 |
Wave I neonatal disorders ACMR with 2 million population |
Baseline |
|
Population increased 100 fold (random seed population size changed from 20k to 2 million) |
||
6.0.3 |
Wave I neonatal disorders ACMR with rate to probability conversion |
Baseline |
|
|||
6.0.4 |
Wave I neonatal disorders ACMR with raw CMSR |
Baseline |
|
|||
6.1 |
Rerun with LBWSG PAF changes for Ethiopia: (1) fix sex-specificity bug in LBWSG PAF calculation, and (2) use LBWSG exposure at birth for calculation of the ENN LBWSG PAF |
All scenarios |
|
|||
6.2 |
Same specifications as model 6.1, but this time with the exponential rate-to-probability conversion (\(p= 1 - e^{(-\text{rate} * \text{duration scaling factor})}\)) in this function |
Baseline |
|
Birth observer updated from output of state table (single row per simulant) to observer detailed in the observer section for all subsequent model runs |
||
6.2.1 |
Same as 6.2, but with a fix for this rate to probability equation transcription error (add back in the duration_scaling_factor) and include abortion/miscarriage/ectopic pregnancy fix to birth observer |
Baseline |
|
|||
6.3 |
Same specifications as model 6.2 (including the exponential rate-to-probability calculation), but with ENN LBWSG PAF updated to use the ENN LBWSG exposure prevalence rather than the LBWSG exposure at birth |
Baseline |
|
|||
6.4 |
Same specifications as model 6.3 (including the ENN LBWSG PAF using ENN exposure), but with the revision of the rate-to-probability calculation back to \(p = \text{rate} * \text{duration scaling factor}\) |
Baseline |
|
|||
6.5 |
|
All scenarios |
|
Default |
Default |
Maternal population observer added for this run and to be included in all subsequent runs |
7.0 |
Wave I neonatal probiotics with scale-up scenarios, same as model 6.0 but with effective coverage (only preterm neonates receive probiotics) |
Baseline and alternative scenarios 2 - 10 |
|
Default |
Stratify probiotics observer (#6) with gestational age above/below 37 weeks for V&V |
Default |
7.0.1 |
Same specifications as 7.0, but with preterm stratification for the probiotics observer included (left out of last run) and fix to the intervention observers to not count stillbirths |
All scenarios |
|
Default |
|
Default |
7.0.2 |
Update \(p_\text{preterm}\) parameter used in the preterm cause model to use birth exposure rather than age-specific exposure |
All scenarios |
|
Default |
Default |
Default |
7.1 |
Update neonatal mortality rates to mortality risks
|
Baseline |
|
Default |
Same modifications as run 7.0.1:
|
Default |
7.1.1 |
Add parameter uncertainty interval for CPAP effect size |
All scenarios |
|
Default |
Same as 7.0.1 |
Default |
8.0 |
Wave I azithromycin |
All scenarios (note new azithromycin scale-up scenario #11) |
|
Default |
Azithromycin stratifications added to observers #1 and #7 (maternal burden and maternal population observers) - to be continued as defaults for all future runs |
Default |
8.1 |
|
Baseline |
|
Default |
Same modifications as run 7.0.1 |
Default |
8.2 |
Update neonatal probiotics intervention effect size in accordance with line #183 in this PR |
All scenarios |
|
Default |
Same modifications as run 7.0.1 |
Default |
8.3 |
Update neonatal antibiotics intervention modeling strategy in accordance with this PR |
All scenarios (note that scenarios #6 and #7 have been deleted as they are no longer relevant and scenario #5 no longer has delivery facility-specific coverage) |
|
Default |
Default |
Default |
9.0 |
Wave I misoprostol |
Baseline and #12 |
|
Default |
Note misoprostol coverage added as a stratifying variable to maternal disorders burden and maternal population observers and delivery facility as a stratifying variable for the maternal disorders burden observer |
Default |
9.1 |
Bugfix to scale up neonatal antibiotics intervention among home deliveries as well |
All scenarios |
|
Default |
Default |
Default |
9.2 |
Larger population size to confirm maternal obstructed labor is not affected by azithromycin |
All scenarios |
|
10x larger population size (100 seeds of 20_000 population size each = 2_000_000 population size per draw) and 2x as many draws for a total of 20 draws |
Default |
Default |
9.3 |
Additional stratifications and updated intervention scenario coverage for intrapartum intervention V&V |
All scenarios – Note changes to scenario numbers 11 and 12 |
|
Same population size as 9.2 |
Make sure maternal disorders burden is stratified by delivery facility and pregnancy outcome as specified |
Default |
10.0 |
Postpartum depression added as new maternal disorder cause |
Baseline |
|
Default |
Default |
Note that postpartum depression cause should be added to the maternal disorders burden observer |
10.1 |
Run with no effect between LBWSG risk factor and Neonatal encephalopathy due to birth asphyxia and birth trauma (but keep LBWSG effects on all other outcomes) |
All scenarios |
|
Default |
Default |
Default |
10.2 |
Same as 10.0 but with additional scenario #13 (azithromycin results) |
All scenarios |
|
Default |
Default |
Default |
11.0 |
Add Hemoglobin risk exposure model. Note that this will be the starting point for the larger wave II hemoglobin module, which will be built out in future model runs |
Baseline |
|
Default |
Default |
Default (no new hemoglobin observer required) |
11.1 |
Bugfix to VPH LBWSG refactor to ensure that LBWSG exposure at birth (rather than the early neonatal exposure) is used for initializing LBWSG exposures in the simulation. Note that this VPH refactor was introduced between models 8.2/8.3 and 9.0 and persisted until this run. |
Baseline |
|
Default |
Default |
Default |
11.2 |
Baseline |
|
Default |
Default |
Default |
|
12.0 |
Capped LBWSG RRs and new late neonatal LBWSG PAF calculation, in accordance with vivarium research PR #1681 and subsequent update in PR #1716 |
Baseline |
|
Default |
Default |
Default |
12.1 |
Bugfix to calculation of prevalence of preterm in this equation, to ensure we include categories with an upper bound of 37 weeks |
Baseline |
|
Default |
Default |
Default |
12.1.1 |
Update to LBWSG PAF calculation for the late neonatal age group. In model 12.0, the PAF calculation for the late neonatal age group did not use the PAF as calculated for the early neonatal age group in the determination of mortality among the early neonatal age group (the PAF using capped and interpolated RRs), as specified in the documentation. This model run will update the LNN LBWSG PAF calculation to utilize the custom calculated ENN LBWSG PAF as specified in the documentation. |
Baseline |
|
Default |
Default |
Default |
13.0 |
Baseline |
|
Default |
Default |
Default |
|
13.1 |
|
Baseline |
|
Default |
Default |
Default |
13.2 |
Update to correct bugs in the LBWSG PAF calculation’s implementation of this equation. In earlier model runs, the PAF calculation for late neonates began from age-specific LBWSG prevalence and the mortality-based weighting implemented did not work due to all deaths being excluded by population filters. Instead, in this run, the PAF calculation for late neonates should begin from birth prevalence and properly apply the mortality-based weighting, as documented. |
Baseline |
|
Default |
Default |
Default |
13.3 |
Update to use end-of-ENN LBWSG prevalence for the \(p_\text{preterm}\) for the LNN age group in this equation. Details can be found in the diff of this pull request. |
Baseline |
|
Default |
Default |
Default |
14.0 |
Wave II updates to the antenatal care attendance module |
Baseline |
|
Default |
Default |
Default, note that we would like the 4-category ANC attendance variable observed |
15.0 |
Delivery facility choice model, including updates to the AI Ultrasound module |
Baseline |
|
Default |
Added preterm status and believed preterm status to maternal population observer (#7) |
Default |
15.1 |
Updates to 15.0 to (1) add preterm and believed preterm status to maternal population count observer and (2) fix bug that results in 0% ANC attendance |
Baseline |
|
Default |
Added preterm status and believed preterm status to maternal population observer (#7) |
Default |
16.0 |
Wave I antenatal corticosteroids |
Baseline |
|
Default |
Default, note that we would like additional stratifications based on believed gestational age in the maternal population, births, and neonatal burden observers |
Default |
16.1 |
Facility choice model bugfixes. Same model as 16.0, but with:
|
Baseline and Ultrasound V&V scenario (scenario #20) |
|
Default |
Default, but add believed preterm stratification to maternal population observer |
Default |
16.3 |
Same as model 16.1, but with facility choice model and neonatal mortality bugfixes. Note this is numbered 16.3 because we originally planned to separate these two sets of changes, but did not run them separately. Facility choice model bugfixes:
Neonatal mortality bugfixes:
|
Baseline and ultrasound V&V scenario (scenario #20) |
|
Default |
Default, but with noted stratifications added |
Default |
16.4 |
Bugfix to resolve missing values for the |
Baseline |
|
Default |
Default, but with preterm birth status stratification of neonatal deaths observers |
Default |
16.5 |
Inclusion of low hemoglobin RR for depressive disorders. No need to actually re-run the model, we just need this RR value active in the interactive context for our custom PAF calculations. |
Baseline |
|
Default |
Default |
Default |
17.0 |
Oral iron antenatal supplementation (IFA/MMS), including effects on hemoglobin, birth weight, gestational age, and stillbirth. See the hemoglobin module for additional detail. Note this intervention has been implemented in previous models such as nutrition optimization. |
Baseline and MMS scale-up scenarios |
|
Default |
Default, note IFA/MMS coverage added as a stratifying variable to maternal population observer. Also add preterm birth stratification to the births observer. |
Default |
18.0 |
Anemia screening implementation (including hemoglobin and ferritin screenings), see also the hemoglobin module |
Baseline, MMS scale-up, and anemia screening scale-up scenarios |
|
Default |
Default, note hemoglobin and ferritin screening coverage and results added as stratifying variables to maternal population observer |
Default |
18.1 |
Model 17.0 bugfixes:
|
No run necessary, all V&V done in the interactive simulation |
N/A |
N/A |
N/A |
N/A |
18.2 |
Model 17.0 bugfixes, continued:
|
No run necessary, all V&V done in the interactive simulation |
N/A |
N |
N/A |
N/A |
18.3 |
Run with updated observer requests to avoid >15 stratifications and multiple bugfixes laid out in the outstanding V&V issues table in this PR |
Baseline, MMS scale-up, and anemia screening scale-up scenarios |
|
Default |
Default |
Default (note that observer 7 has been broken up into 7a and 7b) |
18.4 |
Updated scenarios (this run to be used for presentation to GF and for record of results pre-GBD 2023 update for comparison) |
Scenario numbers 1-9 (all scale-up scenarios for implemented interventions other than misoprostol and hemoglobin-related interventions) |
|
Default |
Default |
Default |
19.0 |
GBD 2023 Update, part 1: data directly from GBD.
This is an artifact only; the model will not run with this artifact, because it is missing required keys. |
All |
|
Default |
Default |
Default |
19.0.1 |
Artifact tweaks and bug-fixes:
Note this is still just an artifact, and not a model run. |
All |
|
Default |
Default |
Default |
19.1 |
GBD 2023 Update, part 2: data derived from GBD through more complex, research-owned processes. |
All |
|
Default |
Default |
Default |
19.1.1 |
Rerun of 19.1 with artifacts that resolved data issue in keys dependent on the BEMONC/CEMONC fraction (that were accidentally run on data specific to model 20.0) |
Baseline |
|
Default |
Default |
Default |
19.1.2 |
Rerun of 19.1.1 with LBWSG PAFs recalculated using capped RRs |
Baseline |
|
Default |
Default |
Default |
20.0 |
In-hospital (CEmONC) delivery estimates from HS team. See PR with diff here |
Baseline |
|
Default |
Default |
Default |
20.0.1 |
Bugfixes from 20.0 (non-zero neonatal deaths and updated intrapartum azithromycin intervention PAF values) |
Baseline |
|
Default |
Default |
Default |
20.0.2 |
Fixes to issues in delivery facility model from 20.0.1 |
Baseline |
|
Default |
Default |
Default |
20.1 |
Sensitivity analysis run: to get an upper bound on the potential impact of AI ultrasound, set the standard deviation of gestational age error to 70 days for “no ultrasound”, 30 days for “standard ultrasound”, and 2 days for “AI ultrasound”. Note that this change should be a one-off, and not built on top of for the next model run. |
Baseline; AI-assisted ultrasound scale-up; CPAP and ACS scale-up; CPAP, ACS, and AI-ultrasound scale-up |
|
Default |
Default |
Default |
20.2 |
Update to >=24 week stillbirth estimates for SBR. See pull request. |
Baseline |
|
Default |
Default |
Default |
21.0 |
Larger run for neonatal mortality V&V with “neonatal all-cause mortality risk”, “neonatal cause-specific mortality risks”, and “impossible neonatal CSMRisk” observers. |
Baseline |
|
For this run only, 10,000,000 population size per draw |
Default |
Default, note addition of “neonatal all-cause mortality risk”, “neonatal cause-specific mortality risks”, and “impossible neonatal CSMRisk” observers. |
22.0 |
Pregnancy model refactor, bringing model up to date with the updated hemoglobin module docs and fixing model 18.3 bugs related to multiple instances of hemoglobin and LBWSG variables that were being inconsistently referenced by different simulation components (See outstanding model verification and validation issues table for full list) |
Baseline, MMS scaleup, and anemia screening scaleup scenarios |
model22.0 |
Default |
Default |
Default |
23.0 |
Inclusion of the residual maternal disorders and abortion/miscarriage/ectopic pregnancy maternal disorders cause models |
Baseline |
|
Default |
Default |
Default |
24.0 |
IV iron intervention coverage and effect on hemoglobin. See the hemoglobin module document for more detail. |
Baseline and IV iron scale-up scenarios |
|
Default |
Default, note IV iron coverage as a new stratifying variable to the maternal population observer |
Default |
25.0* |
IV iron effects on birth weight, gestational age, and stillbirth as defined on the IV iron intervention document (data specific to GBD 2023 has yet to be generated) |
Baseline and IV iron scale-up scenarios |
|
Default |
Default |
Default |
26.0* |
Updated hemoglobin effects as defined on the hemoglobin risk effects document (Custom PAFs and neonatal sepsis effects have yet to be calculated for GBD 2023)
|
Baseline and IV iron scale-up scenarios |
|
Default |
Default |
Default |
27.0 |
Postpartum hemoglobin |
Baseline, MMS scale-up, and IV iron scale-up scenarios |
|
Default |
Default |
Default |
28.0 |
Anemia YLDs |
Baseline, MMS scale-up, and IV iron scale-up scenarios |
|
Default |
Default |
Default, note new anemia YLD observer |
29.0* |
Effects of maternal hemorrhage (and possibly maternal sepsis) on postpartum hemoglobin. Model run is blocked by the following research tickets (1) update maternal hemorrhage risk effect docs to GBD 2023 and consider adding risk effect for maternal sepsis |
Baseline, MMS scale-up, and IV iron scale-up scenarios |
|
Default |
Default |
Default |
Note
Some of the notebook URLs for the older runs might be out-of-date. If you click one of these links and it gives you a 404 error, add to your URL /old_vnv_notebooks/ after verification_and_validation, and that should take you to the right place!
Model number |
V&V plan |
V&V summary |
Link to notebook |
|---|---|---|---|
1.0 |
|
All checks passed except last one; RT is updating our observer output requests to add an observer for pregnant person age. |
|
2.0 |
|
All checks passed except error found in GBD 2021 for Pakistan fistula modeling - need to update the artifact for Pakistan OL prevalence values from GBD 2021 to GBD 2023. Did not explicitly check YLLs yet. |
|
3.0 |
|
Found an error in LBWSG distribution in artifact, which might be the cause of some of the other checks that weren’t passing, including the ACMR for the late neonatal group and the CSMR for preterm |
|
3.1 |
Validate LBWSG exposure distribution |
LBWSG distributions in artifact, GBD, and simulation are now matching, but preterm deaths still look too low in the simulation |
|
3.2 |
Validate all-cause mortality for early and late neonatal age groups with LBWSG component removed |
Early neonatal mortality is still being overestimated in the simulation |
|
3.3 |
|
Early neonatal mortality is validating now! Note: Ali noticed in the LBWSG interactive sim that the state table and pipeline values for LBWSG exposure don’t match, but engineers confirmed this is okay, the pipeline values refresh after being recorded in the state table (and then are not used again). |
|
4.1 |
Validate RR of CPAP on RDS preterm (and confirm other causes are unchanged) |
Cannot validate, need observer with counts per facility type |
|
4.2 |
Validate RR of CPAP on RDS preterm (and confirm other causes are unchanged) |
Cannot validate, need to add delivery facility column in births observer and stratification for CPAP availability |
|
4.3 |
Validate RR of CPAP on RDS preterm (and confirm other causes are unchanged) |
Not validating, need to update how we determine which delivery facility type a simulant will go to |
|
4.4 |
Validate RR of CPAP on RDS preterm (and confirm other causes are unchanged) |
Not validating, we are seeing negative mortality rates for Other causes |
|
4.5 |
Validate RR of CPAP on RDS preterm (and confirm other causes are unchanged) |
CSMRs and ACMR are all validating now, with the bugfix to adjust all negative values to 0 and rescale the rest of the RRs to add up to 1 |
|
4.7 |
Validate abortion/miscarriage/ectopic pregnancy duration is between 6 and 24 weeks and uniformly distributed. |
Validated for all 3 locations |
|
5.0 |
Validate RR of antibiotics on sepsis (and confirm other causes are unchanged) |
Everything is validating - RR on sepsis aligns with expected value; other causes, non-RDS preterm, and encephalopathy all have the expected RRs of 1 from antibiotics. There’s an RR of 0.78 for antibiotics on preterm with RDS, but we confirmed that when we group this by facility type, there is the expected RR of 1. This is because the probability of a simulant receiving CPAP and the probability of receiving antibiotics are not independent (both related to facility choice). |
|
5.1 |
Validate maternal and neonatal disorders and intervention effect sizes after refactor |
Everything is validating! We noticed the maternal disorders incidence parquet files were mislabeled, the fix for that has already been implemented. |
|
6.0 |
Validate coverage, RR of probiotics on sepsis (and confirm other causes are unchanged) |
Neonatal ACMR looks off, residuals have gotten increasingly worse with additional interventions |
|
6.0.1 |
Validate neonatal disorders ACMR with 200k population without interventions |
Used the attached notebook and spreadsheet to figure out which runs were validating with ACMR and which were not |
|
6.0.2 |
Validate neonatal disorders ACMR in baseline scenario with 2 million population |
Used the attached notebook and spreadsheet to figure out which runs were validating with ACMR and which were not |
|
6.0.3 |
Validate neonatal disorders ACMR when reverting the rate to probability conversion for mortality rates when choosing when neonates die |
Used the attached notebook and spreadsheet to figure out which runs were validating with ACMR and which were not |
|
6.0.4 |
Validate neonatal disorders ACMR when using raw CSMRs for the non-preterm neonatal causes, removed LBWSG RRs on those neonatal causes |
Used the attached notebook and spreadsheet to figure out which runs were validating with ACMR and which were not |
|
6.1 |
Check ENN mortality ratio compared to GBD |
Neonatal mortality ratios are now slightly underestimated (rather than the previous overestimation). Note that calculation of the mortality ratio of the LNN age group has been updated in this notebook to be [deaths in LNN age group] / [population at the start of the LNN age group], rather than a denominator of live births so that LNN mortality is not dependent on ENN mortality. |
|
6.2 |
Check ENN mortality ratio compared to GBD |
Neonatal mortality ratios are now dramatically overestimated. Note that while the birth observer has changed between models 6.1 and 6.2, it has been verified that birth counts do not vary between these runs and that greater death count values are driving the difference between neonatal mortality ratios in 6.1 and 6.2 |
|
6.2.1 |
Check ENN mortality ratio compared to GBD, check that birth observer is recording abortion/miscarriage/ectopic pregnancies |
|
|
6.3 |
Check ENN mortality ratio compared to GBD and models 6.1-6.4 |
Mortality is slightly overestimated. It appears that overestimation in 6.3 is slightly larger in magnitude than the underestimation of 6.1. |
|
6.4 |
Check ENN mortality ratio compared to GBD and models 6.1-6.4 |
Mortality is overestimated to a degree greater than 6.3 |
|
6.5 |
|
|
|
7.0 |
|
|
|
7.0.1 |
|
All specified V&V criteria looks great! Did notice that CPAP relative risk in artifact is a point value despite having uncertainty specified in documentation. |
|
7.0.2 |
Check that preterm birth mortality is as expected: we should change from a slight overestimation to a slight underestimation. A slight underestimation is expected due to known mortality probabilities greater than 1, which will be addressed in future model runs. |
The overestimation of preterm birth mortality is of lower magnitude than in 7.0.1, indicating that the update of the preterm prevalence term improved the model. However, preterm birth mortality remains slightly overestimated on average rather than the expected slight underestimation. |
|
7.1 |
|
|
|
7.1.1 |
|
All looks good except the artifact values for the CPAP relative risk are not quite as expected due to issue raised in this comment |
|
8.0 |
|
|
|
8.1 |
|
|
|
8.2 |
|
All looks good! |
|
8.3 |
|
All looks good, except antibiotics coverage is not being scaled up among those who deliver at home as it should be |
|
9.0 |
|
|
|
9.1 |
|
|
|
9.2 |
|
Same conclusions as 9.0 |
|
9.3 |
Confirm intrapartum interventions are meeting V&V criteria |
Intrapartum intervention coverage and effects are looking just as expected :) |
|
10.0 |
|
All looks great! |
|
10.1 |
Check if cause-specific neonatal mortality validates |
|
|
10.2 |
Confirm baseline mortality is as expected, scenario-specific intervention coverage is as expected |
Looks as expected (including persistent NN mortality underestimation that arose in model 9.0) |
|
11.0 |
|
All looks good! However, we are not using the draw numbers pre-specified in this PR. The draws that have been run include duplicate hemoglobin exposure values. |
|
11.1 |
|
Looks good! |
|
11.2 |
Check that draw numbers have been updated |
Looks good! |
|
12.0 |
|
|
|
12.1 |
|
Neonatal cause-specific mortality risks match expectation for both preterm and non-preterm causes in the early neonatal period. We appear to be systematically underestimating preterm CSMRisks in the late neonatal period. |
|
12.1.1 |
|
|
|
13.0 |
|
|
|
13.1 |
|
|
|
13.2 |
|
|
|
13.3 |
|
|
Model 13.3 neonatal checks Model 13.3 interactive sim neonatal mortality checks |
14.0 |
|
All V&V criteria met! |
|
15.0 |
Checks using observer outputs:
Checks using interactive sim:
|
Measures meeting V&V criteria:
V&V issues:
Not able to be checked:
|
|
15.1 |
Same as 15.0 |
Measures meeting V&V criteria:
Known issues:
V&V targets not met: (thought to be related to “known issues”)
|
|
16.0 |
|
|
|
16.1 |
|
All V&V criteria met except for:
(Note that scenario #20 was not included in this run, so related V&V will be performed in 16.3 instead) |
|
16.3 |
For facility choice: Same as 16.1 and 16.0 For neonatal mortality:
|
|
|
16.4 |
Same as 16.3 |
|
|
17.0 |
|
|
|
18.0 |
|
|
Interactive simulation notebook for model 18.0 found here. Note that simulation results for this run were not generated due to too many observer stratifications. |
18.1 |
|
|
|
18.2 |
Same as 17.0 |
|
|
18.3 |
Same as 17.0 and 18.0 |
Meeting the following criteria:
Partially meeting the following criteria:
Not meeting the following criteria:
|
|
19.1 |
|
|
|
19.1.1 |
Same as 19.1 and confirm specific issues from 19.1 are resolved |
|
Model 19.1.1 V&V notebooks Model 19.1.1 interactive sim neonatal mortality V&V notebook |
19.1.2 |
Same as 19.1.1 and confirm specific issues from 19.1.1 are resolved |
||
20.0 (CEMONC data update) |
|
|
|
20.0.1 |
|
|
|
20.0.2 |
|
||
21.0 (neonatal mortality V&V) |
Confirm expected rates of cause-specific and overall maternal disorders causes |
||
22.0 (pregnancy refector) |
Same as 18.3 |
||
23.0 (residual and other maternal disorders causes) |
|
||
24.0 (IV iron coverage and effect on hemoglobin) |
|
||
25.0 (IV iron effects on BW, GA, SB) |
|
||
26.0 (updated hemoglobin effects) |
|
||
27.0 (postpartum hemoglobin) |
In the interactive simulation, confirm postpartum hemoglobin exposure matches hemoglobin exposure at the end of pregnancy for simulants who survive to the postpartum period |
||
28.0 (anemia YLDs) |
|
||
29.0 (maternal disorders effects on postpartum hemoglobin) |
|
Issue |
Explanation |
Action plan |
Timeline |
|---|---|---|---|
Maternal disorders burden does not vary by scenario despite increased coverage of the oral iron intervention affecting hemoglobin exposure |
It appears that the |
Engineers to address during pregnancy model refactor |
Pregnancy refactor model 22.0 |
Neonatal deaths do not vary by scenario despite increased coverage of the oral iron intervention that should affect BW and GA exposures (and therefore child mortality) |
Unknown, verified impacts of oral iron intervention of birth weight and gestational age pipeline values in the interactive simulation. Ali suspects that this issue is related to LBWSG RRs being assigned either based on the state table exposure values (that are not affected by the interventions) or after LBWSG exposures get reset in pipeline values and maybe lose the impact of the interventions |
Engineers to address during pregnancy model refactor |
Pregnancy refactor model 22.0 |
No impact of IFA or MMS on observed preterm birth counts |
Ali is verifying expected effects of IFA and MMS on preterm birth assessed by the gestational age pipeline values in the interactive simulation. Ali suspects that while we have the interventions modifying the pipeline values for these exposures, we are observing preterm birth based on the state table values that are not being modified by interventions. |
Engineers to address during pregnancy model refactor |
Pregnancy refactor model 22.0 |
No impact of MMS on stillbirth |
Unknown, was previously meeting verification criteria. No impact in the interactive sim or in the simulation results |
Engineers to investigate and update |
Anemia screening bugfix run, version number TBD |
Ferritin screening rate < 100% among eligible population in scale-up scenario |
We are only testing ferritin among those who have low exposure values for their tested hemoglobin AND their true hemoglobin. Everyone who has a low tested hemoglobin exposure should be screened for ferritin regardless of their true hemoglobin exposure |
Engineers to address during pregnancy model refactor |
Pregnancy refactor model 22.0 |
Hemoglobin screening test and anemia status during pregnancy appear to be reading in an inappropriate hemoglobin exposure measure |
See linked comments (it appears we created a new measure to be used in these instances, but did not actually update it as the input variables) |
Engineers to address during pregnancy model refactor |
Pregnancy refactor model 22.0 |
Propensity for LBWSG category remains constant across timesteps, but propensity for continuous BW and GA values reset at each timestep |
This should not cause significant bias in our results, but it is not logical to have a different birth weight at different ages and unnecessarily increases stochastic uncertainty in our simulation |
Engineers to address during pregnancy model refactor |
Pregnancy refactor model 22.0 |
There is non-zero coverage of hemoglobin screening among those who attend first trimester screening ONLY |
This is inconsistent with documentation (hemoglobin screening should occur at later pregnancy ANC visit only) |
Engineers to address during pregnancy model refactor |
Pregnancy refactor model 22.0 |
Ali’s documentation issue resulted in known issues with ferritin data used for implementation of anemia screening model |
Either update to strategy outlined in this PR or an alternative strategy using PRISMA data shared by the Gates foundation |
Will decide how to proceed when we receive PRISMA data |
|
Unable to verify ferritin screening results among those who are not anemic according to hemoglobin level at the time of testing |
Re-address when we update ferritin exposure model |
Maintain existing behavior for now |
TBD |
Current implementation is based off of an adaptation of the assumptions used in the GBD 2021 major depressive disorders cause model |
We will need to either (1) update our model to be in line with the GBD 2023 model and consider updating our PAF calculation strategy as described in this ticket, or (2) update to the extra-GBD data on peripartum depression obtained from the mental disorders modelers |
Will decide how to proceed after discussing with the mental disorders modelers |
|
Miscalibration of maternal sepsis incidence rates, particularly for Nigeria |
Thought to be due to using the fatal PAF from GBD applied to incidence and/or the location-aggregated PAF for our modeled locations which are not most detailed locations |
Update to custom-calculated PAF and reassess |
TBD |
Late neonatal mortality due to preterm birth slightly underestimated and other-causes mortality may be slightly overestimated (though within 10%) |
Unknown – possibly related to negative other causes mortality in Pakistan and Nigeria. |
Zeb to request an observer for negative other causes mortality |
Model 20.0 |
Scenario with increased ultrasound coverage leads to (very slightly) lower IFD |
Does not appear to be an implementation bug (all facility choice model V&V criteria are met), but is not the expected result |
Ali to investigate the rates of false positive and false negatives by scenario to determine if ultrasound improvements is reducing false positives among term babies more than it is reducing false negatives among preterm babies, which could explain this result |
Tabled for now. See ticket here |
Late neonatal mortality due to preterm birth with RDS slightly (~2%) underestimated |
The PAF of ACS and CPAP on preterm birth with RDS CSMRisk is calculated with delivery facility proportions at birth, not at 7 days |
Accept this limitation, until/unless there are other reasons to revamp PAF calculation, since this would require many components not currently present in PAF sim |
N/A |
Early neonatal mortality due to preterm birth with RDS slightly (~1.5%) overestimated and late neonatal mortality slightly (~0.75%) underestimated across all causes |
The PAF of ACS and CPAP on preterm birth with RDS CSMRisk is calculated without accounting for correlation between LBWSG and CPAP/ACS, which is induced by the facility choice model. The miscalibration in ENN causes miscalibration of LBWSG exposure for LNN. |
Accept these limitations, until/unless there are other reasons to revamp PAF calculation, since this would require many components not currently present in PAF sim. Note that the LNN limitation stacks with the previous limitation for preterm birth with RDS to result in a nearly 3% underestimate in that LNN CSMRisk. |
N/A |
In GBD data for Pakistan (for both GBD 2021 and 2023 rounds) the values for incidence, prevalence, and YLDs of rectovaginal fistula (s_189) and vesicovaginal fistula (s_190) sequelae of the maternal obstructed labor and uterine rupture cause (c_370) are zero, causing unexpectedly low YLDs for the obstructed labor and uterine rupture cause (~10 times fewer YLDs than India despite incidence being only about twice as low) |
Unknown, appears to be an issue with the GBD model |
Research to consider how to handle this: remain consistent with GBD or use similar location (India?) as a proxy location for YLDs per obstructed labor case? |
TBD |
6.0 Limitations
Unclear if we will be able to include upstream factors, but these are likely correlated with many things such as ANC visit rate, care available, or even outcome rates
We currently do not consider the potential impact of pregnancy outcome, mode of delivery, or preterm status on postpartum depression incidence (although we do model the impact of hemoglobin on PPD incidence). This may cause us to underestimate the impact of interventions that work through these mechanisms on postpartum depression burden.
Factors such as birth asphyxia have been shown to predisopose infants to infection which can result in sepsis [Tikmani-et-al-2016]. We do not model a relationship between birth asphyxia and sepsis, so we do not capture any indirect effects of interventions to reduce birth asphyxia (like cesarean sections) on sepsis as mediated through reductions in birth asphyxia.
We assume that all maternal deaths occur at the conclusion of the intrapartum period and prior to the start of the postpartum period. Therefore, we assume it is not possible for any simulants who die of a maternal disorder to experience postpartum YLDs (such as those due to postpartum depression and/or postpartum anemia). However, this may be possible in reality, particularly for those who die of “late maternal deaths.”
We track certain outcomes among abortion/miscarriage/ectopic pregnancies in this model, including first trimester ANC attendance and associated interventions, anemia YLDs, and postpartum depression. However, these pregnancies are not given special consideration other than their premature end and we do not consider how this population may differ from pregnancies that end in live or still births in terms of their ANC attendance rates or other attributes beyond maternal disorders burden. Additionally, we do not model any variation in these attributes by subtype (abortion vs. miscarriage vs. ectopic pregnancy), despite there being expected differences in behavior between these groups.
We do not model an underlying correlation between hemoglobin exposure and stillbirth rates, despite evidence that such an association exists. Therefore, our IV iron intervention model, which is targeted to those with low hemoglobin, will be misaligned with respect to the stillbirth rate among the IV iron intervention target population.
We could use the GBD risk effects between hemoglobin and stillbirth to model baseline correlation only and not model updates in stillbirth rates in response to changes in hemoglobin exposure to address this limitation (as these effects are captured in the impact of the hemoglobin-affecting interventions IV Iron and IFA/MMS already). However, this model upgrade is not highest priority. See this backlog JIRA ticket #2343
[Finkelstein-et-al-2024] primarily includes RCTs from high-income countries, so the effect size for IFA on maternal hemoglobin may be overestimated for Sub-Saharan African countries (including Ethiopia and Nigeria) with typically higher rates of non-iron deficiency anemias.
We do not currently model an oral iron treatment intervention, despite the recommendation by WHO to treat all pregnancies with IFA and all anemic pregnancies with oral iron treatment (essentially a higher dosage of iron than IFA). We have a JIRA ticket to add this intervention in the future, but it is not currently prioritized. There are some individuals who receive oral iron treatment at baseline and we want to model the replacement of that oral iron treatment with IV iron treatment. However, we are not subtracting out the effect of oral iron treatment prior to modeling the scale up of IV iron treatment. This will result in the following limitations:
For individuals who received oral iron treatment at baseline and still remain eligible for IV iron following their oral iron treatment: we will double count the impact of the interventions, thus overestimating the potential scale-up of IV iron.
For individuals who received oral iron treatment at baseline and no longer remain eligible for IV iron following their oral iron treatment: there will be essentially no difference in impact for this population given that IV and oral iron treatment have basically equal impacts, however, we will be underestimating the size of the population requiring treatment and therefore underestimating the cost required to achieve the health outcomes seen in these scenarios.
7.0 References/Other
See the “(“Darmstadt 2011” reference in: Tikmani SS, Muhammad AA, Shafiq Y, Shah S, Kumar N, Ahmed I, Azam I, Pasha O, Zaidi AK. Ambulatory Treatment of Fast Breathing in Young Infants Aged <60 Days: A Double-Blind, Randomized, Placebo-Controlled Equivalence Trial in Low-Income Settlements of Karachi. Clin Infect Dis. 2017 Jan 15;64(2):184-189. doi: 10.1093/cid/ciw690. Epub 2016 Oct 19. PMID: 27941119; PMCID: PMC5853586.
Note
This concept model was reorganized in April 2025 after much of wave I had been implemented. A record of the PRs for this reorganization are listed below:
Pregnancy component reorganization: https://github.com/ihmeuw/vivarium_research/pull/1615
Intrapartum component reorganization: https://github.com/ihmeuw/vivarium_research/pull/1617
Neonatal component reorganization: https://github.com/ihmeuw/vivarium_research/pull/1619